90% of U.S. adults age 65+ have at least one chronic condition
75% ages 35–64 have at least one condition
60% ages 18–34 have at least one condition
42% have 2 or more chronic conditions
12% have 5 or more chronic conditions
Augmenting in-office visits with at-home Telehealth Solutions
provide patients with access to the resources they need
to effectively manage their chronic conditions





Our Telehealth Professionals monitor patient’s physiological and non-physiological data daily!
Patients, family, and caregivers can text, call, and email their Telehealth Professional.
High-touch communication is how we take patient adherence to a new level!


CCM brings structure to patient care delivered remotely – between office visits. Designed for patients “with two or more chronic conditions expected to last at least 12 months or until the patient’s death, and place the patient at significant risk of death, acute exacerbation, or functional decline.”
Medicare introduced CCM more than ten years ago to incentivize healthcare providers to maintain monthly contact with patients by phone, email, and text. This high-touch, remote care model has proven effective at early detection, early intervention, reduced visits to the ER, reduced hospital admissions, and generally improved patient outcomes.

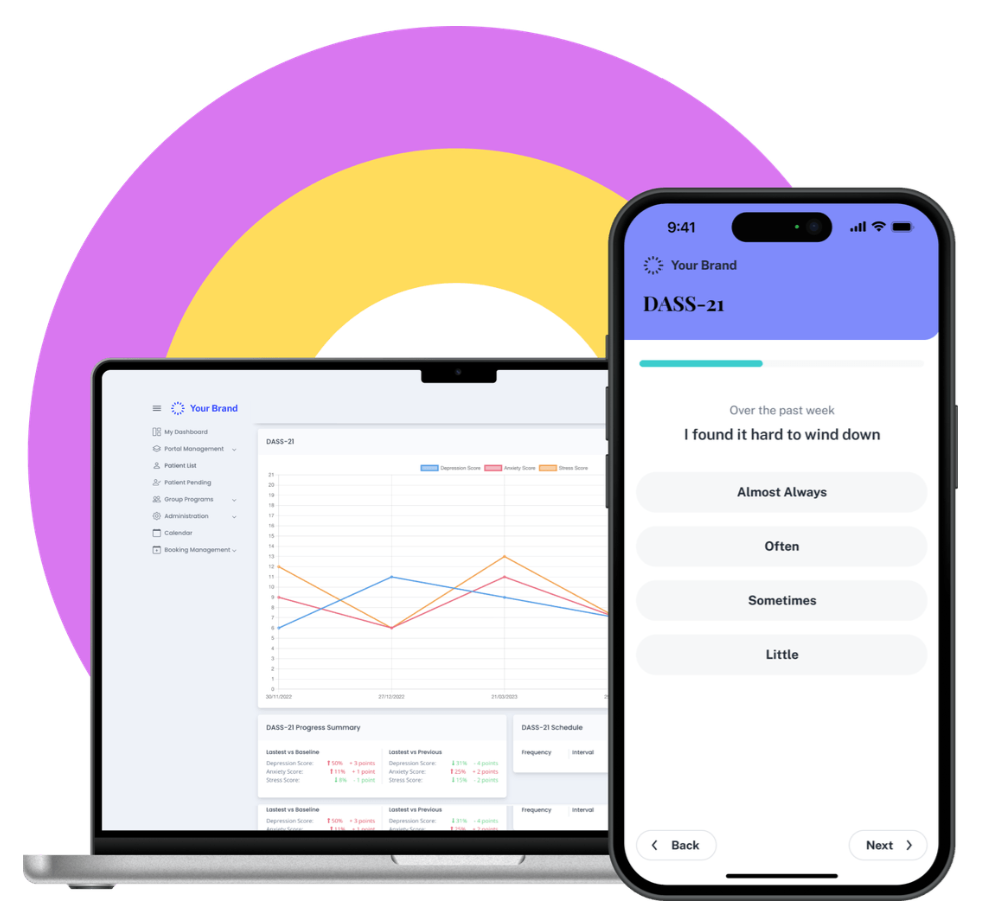
RTM relies on mobile apps to remotely monitor and manage patients from the comfort of their home. Remote care teams communicate with patients daily to assess non-physiological patient-reported data.
These include medication adherence, response to therapy, pain/mood/symptom tracking, and more.
These data provide critical insights into which therapies and medications are working or not working.
By informing care decisions in real time, physician-led care teams intervene early to improve outcomes.

RPM monitors patients remotely using an FDA-cleared device capable of collecting physiological data (Blood Pressure, Blood Glucose, SpO2, weight loss/gain, and temperature) at home and electronically transmitting those data to your care team at a different location. Your remote care team will monitor each patient’s incoming readings daily, call each patient by phone monthly, and communicates with patients, family, caregivers, and physician-led care teams throughout each month.

PCM is a set of non face‑to‑face care management services for patients with a single serious or a high‑risk chronic condition. The condition must be expected to last at least 3 months and require focused, ongoing management and coordination by one clinician. PCM is similar to CCM but is centered on one primary condition vs 2+ conditions.


Medicare, Medicare Advantage, and Most Private Payors cover the cost of CCM, RPM, PCM, and RTM.
87% of Medicare recipients have some form of supplemental coverage i.e., Medigap, Medicaid, Employer.
Almost 9 out of 10 Medicare patients can enroll in Telehealth Services without the burden of a co-pay

RPM, CCM, RTM, and PCM are pivotal tools that helps bridge the home-office divide.
Individual health data are collected outside the office setting and transmitted to care teams. Informed, Physician-led care planning facilitates more optimal disease management.
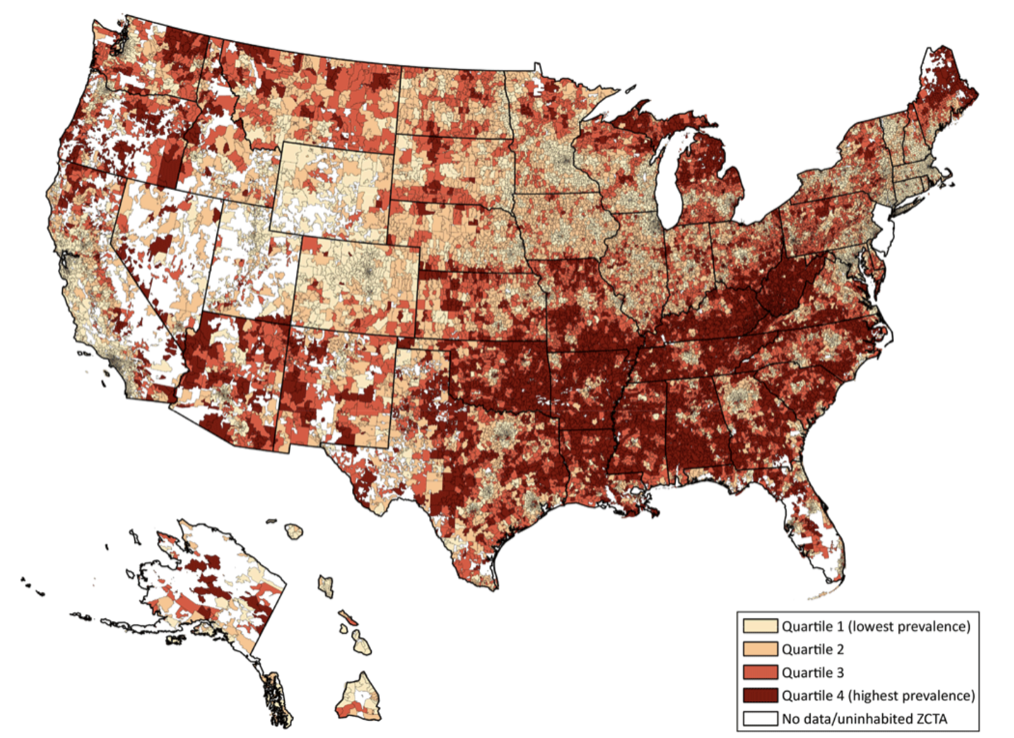
The State of RPM for Chronic Disease Management in the U.S.
J Med Internet Res 2025;27:e70422 URL: https://www.jmir.org/2025/1/e70422 DOI: 10.2196/70422
Mayo Clinic
Adherence to prescribed medications is associated with improved clinical outcomes for chronic disease management and reduced mortality from chronic conditions.
Conversely, non-adherence is associated with higher rates of hospital admissions, suboptimal health outcomes, increased morbidity and mortality, and increased health care costs.
Physician-led Remote Care Teams monitor patient’s
Physiological and Non-Physiological health – daily


Medical Group Practices can augment in-office care with our Remote Telehealth Care Teams.
Our remote clinical and administrative resources enable more time for in-office patient care.
This reduced in-office workload results in higher employee satisfaction and retention.
PRIMARY CARE
INTERNAL MEDICINE
CARDIOLOGY
RESPIRATORY & PULMONOLOGY
ENDOCRINOLOGY
NEPHROLOGY
OPHTHALMOLOGY
NEUROLOGY
ONCOLOGY
MENTAL/BEHAVIORAL HEALTH
GASTROENTEROLOGY
OB/GYN
ORTHOPEDICS
PHYSICAL THERAPY CENTERS
PAIN CLINICS
CHRIROPRACTIC MEDICINE
WEIGHT LOSS SPECIALISTS
SKILLED NURSING FACILITIES
ASSISTED LIVING FACILITIES
PODIATRY